
Contents
- Introduction: State Of Emergency
- Phase 3: The Human Guinea Pig
- First Do No Harm (A Quick Look At Some Novel "Vaccine" Tech)
- Is There An Emergency? (Data & Context)
i. All Cause Mortality (Deaths) in England & Wales 1900 - 2020
ii. All Cause Mortality (Deaths) in England & Wales 1971 - 2020
iii. All Cause Mortality (Deaths) of English & Welsh Residents 2017 - 2020
iv.. Age Adjusted (WHO) All Cause Mortality (Deaths) in England: 2001 - June 2021
v.. Hospital Bed Occupancy in England (Year-End 2019 vs 2020)
vi. Deaths (All Causes) in England & Wales vs COVID-19 "Cases" (+PCR Tests) - RT-PCR, The Pandemic Machine
i. What is PCR?
ii. What is a Case?
iii. PCR Amplification Cycle Threshold (Ct) & False Positives
iv. The Corman-Drosten RT-qPCR: A "Useless Test" Yields Meaningless Data
v. The Data is False, The Consequences are Real - The Asymptomatic Spreader
- A Viral PR Machine
i. A Brief History (H1N1)
ii. Fast Forward to 2020
iii. Viral Public Relations
iv. Qui Bono - The Future Died In Someone's Past (Collateral "Vaccine" Damage?)
i. The "Knowns" and the "Known Unknowns"
ii. Light at the End of the Tunnel (Crimes & Revelations) - Changelog (Amendments, Corrections, Additions)
1) Introduction: State Of Emergency
The premature and express roll-out of experimental unlicensed "vaccines" to supress mild to moderate symptoms of the COVID-19 disease (rather than provide immunity or prevent transmission of the SARS-CoV-2 virus) is premised on the idea that we're in the midst of a global pandemic; a medical emergency.
Regulation 174 of the UK's 2012 Human Medicines Regulations was amended on October 16th 2020 (adding 174A) to enable the temporary authorisation of unlicensed medicines (including vaccines) in response to a public health emergency.
Before we look at whether this emergency necessitates mass human experimentation, let's first look at the "vaccines" and the scarce data from the trials. We'll start with the latter, since many think the trials are behind us, though as you'll see, they absolutely are not.
2) Phase 3: The Human Guinea Pig
On the 8th December, the BBC reported: "The Oxford/AstraZeneca Covid vaccine is safe and effective, giving good protection, researchers have confirmed". The Lancet study they were referencing actually stated: "ChAdOx1 nCoV-19 has an acceptable safety profile and has been found to be efficacious against symptomatic COVID-19 in this interim analysis of ongoing clinical trials".
Iain Davis, in an excellent piece titled, "What Vaccine Trials?" (published on Off-Guardian, 3rd Jan 2021 and excerpted below), clearly lays out the trial phases and their end-points and states categorically:
"[...] If you decide to have Pfizer and BioNTech’s experimental mRNA-based BNT162b2 (BNT) vaccine, or any other claimed COVID 19 vaccine for that matter, you are a test subject in a drug trial.
[...] The regulators and governments have worked with the pharmaceutical corporations to conflate the limited data from the initial, or phase one trials with the incomplete and ongoing data collection from the substantially larger phase two and three trials. The MSM [mainstream media] have then falsely claimed the 1,2,3 phase trials are complete and insinuated that the untested data demonstrates vaccine efficacy and safety. In reality, not only has the reporting of existing data been manipulated to show efficacy that isn’t evident in the raw data itself, the most important and meaningful phases of the trials have barely begun, let alone been completed.
[... AstraZeneca's] AZD1222 was registered with the U.S. Center for Disease Control as clinical trial NCT04516746 [Archived 29th December 2020]. It is incomplete and the estimated end date is February 21st 2023. The CDC state: "No Study Results Posted"
[...] The start date for [Pfizer BioNTech's trial] NCT04368728 was April 29th [2020] and the estimated trial completion date is January 27th 2023. The estimated end date of the primary or phase one of a three phase trial is June 13th 2021.
Informed consent is a legal obligation and providing false or incomplete information to gain consent for vaccination (or any medical procedure) is a crime. Are recipients being told these "vaccines" are experimental (and don't prevent infection or transmission) and that they are consenting to participate in a pharmaceutical trial?
While we remain unsure of their safety, editor of the British Medical Journal (BMJ), Peter Doshi gleaned enough from the limited data released so far to derive a relative risk reduction for Pfizer and Moderna's "vaccines" between 19% and 29% (not 95% as the respective companies had stated via press release, see "Pfizer and Moderna’s “95% effective” vaccines - we need more details and the raw data").
The absolute risk reduction (ARR), using Pfizer's own figures is 0.84%:
The absolute risk of developing COVID 19 symptoms without the vaccine is supposedly 0.88% and with the vaccine 0.044%. In absolute terms, the effectiveness of the vaccine is (0.88-0.044)%. A risk reduction of 0.84%.
Later, we'll explain why even these numbers and all data that has guided mask mandates [PDF], lockdown policies and even the COVID-19 "vaccine" trials, are largely meaningless. But before we do, let's look at the "vaccines" themselves.
3) First Do No Harm (A Quick Look At Some Novel "Vaccine" Tech)
So far, we have an unlicensed experimental "vaccine" technology with an unknown risk profile, that doesn't prevent infection or transmission but may reduce your risk of developing COVID-19 symptoms by up to 0.84% (ARR). With such modest expected benefits, one should hope these novel products at least do no harm.
There are two main differences between the AstraZeneca (AZ) and Pfizer / Moderna "vaccines" (and here I'm going to attempt a lay translation - more detail and a complete list of ingredients are available here):
The Delivery Mechanism (vector)
- The Pfizer / Moderna vaccines use an engineered lipid nano-particle with a PEG (Polyethylene glycol) coating (which seems to be causing anaphylaxis, also see here)
- AZ use a chimpanzee adenovirus to deliver their payload. The vaccine is grown on an "immortalized" (and potentially tumorigenic?) human cell line MRC-5 (genetically engineered and mass produced) from a 1960s aborted foetus (the contaminants are then "purified" away - in theory)
The Payload (code)
- The Pfizer / Moderna vaccines use mRNA (messenger RNA) to encode the cell to "grow" a (SARS-CoV-2-facsimile) spike protein which provokes an immune response facilitating the production of B-Cell antigens (in the hope that if you get the real thing your immune system will recognise the spike protein and provide a rapid response).
- The AZ "vaccine" is similar but uses more robust DNA (which is why it doesn't require the low temperature during transport) to encode the cell to grow a (SARS-CoV-2-facsimile) spike protein.
In essence, both "vaccines" or "gene therapies" are instructing the body to create something the immune system will attack. Traditional vaccines enter the body as foreign agents (either inactivated virus with adjuvants as with the flu vaccine, or small amounts of live attenuated virus as with the Polio vaccine), these novel "vaccine platforms" seem to muddy the water between what the body regards as "external to self" (and thus foreign) and what is "part of self". A dysregulated immune system may attack its host (mistaking it as foreign); we call such pathologies "auto-immune diseases".
Unfortunately, we're beginning to see disturbing evidence of serious adverse events: transverse myelitis (AZ), multiple sclerosis (AZ), Bell's palsy (Pf, Mo) were all evident in the early trials and during the mass roll-out phase of the ongoing trials we've seen Acute Idiopathic Thrombocytopenia Purpura (ITP), neurological disorders like akenesia and dystonia, cardiovascular complications and death (in the healthy as well as the frail and old).
The pharmaceutical companies are currently treating any and all such side effects as coincidences. The statistical evidence that these experimental "vaccines" cause "coincidences" is mounting (and perhaps this disease called "coincidence" should be listed as a potential side effect on the COVID vaccine inserts).
If these truly are coincidences, it would appear that they're coincidences of the expected kind. The FDA (US Food & Drug Administration) is looking out for the following:
 Source: Vaccines and Related Biological Products Advisory Committee October 22, 2020 Meeting Presentation (PDF)
Source: Vaccines and Related Biological Products Advisory Committee October 22, 2020 Meeting Presentation (PDF)
The UK's equivalent to the FDA, the MHRA put out a tender (23/10/20, a day after the above advisory) for an Artificial Intelligence Software System to "process the expected high volume of Adverse Drug Reactions" :
 Source: MHRA Tender on TED for "Software package and information systems" (2020/S 207-506291)
Source: MHRA Tender on TED for "Software package and information systems" (2020/S 207-506291)
So now we've seen the experimental nature of the response to this "unprecedented public health emergency", let's ask a simple, yet forbidden question ...
4) Is There An Emergency?
Here we're going to look at data for England & Wales and see if we can find an emergency. We'll start from a historical, bird-eye view and apply a temporal zoom as we go. The historical data series are adjusted for population growth (i.e. deaths per 100,000 of population).
1. All Cause Mortality (Deaths) in England & Wales 1900 - 2020
 Source: Alliance for Natural Health (Data: Office of National Statistics, note: the "England & Wales Mortality" series does not include the deaths of nationals overseas or service personnel that died abroad)
Source: Alliance for Natural Health (Data: Office of National Statistics, note: the "England & Wales Mortality" series does not include the deaths of nationals overseas or service personnel that died abroad)
So yes, there's an uptick, but we didn't shut down the economy, lock down the population, don masks and conduct mass human experiments during the flu seasons of 1951 and 1968 and we're barely back to where we were in 2003 (a year when two million people protested the Iraq war in London; but not a year remembered for over-flowing morgues - at least not in the UK).
Let's zoom in.
2. All Cause Mortality (Deaths) in England & Wales 1971 - 2020
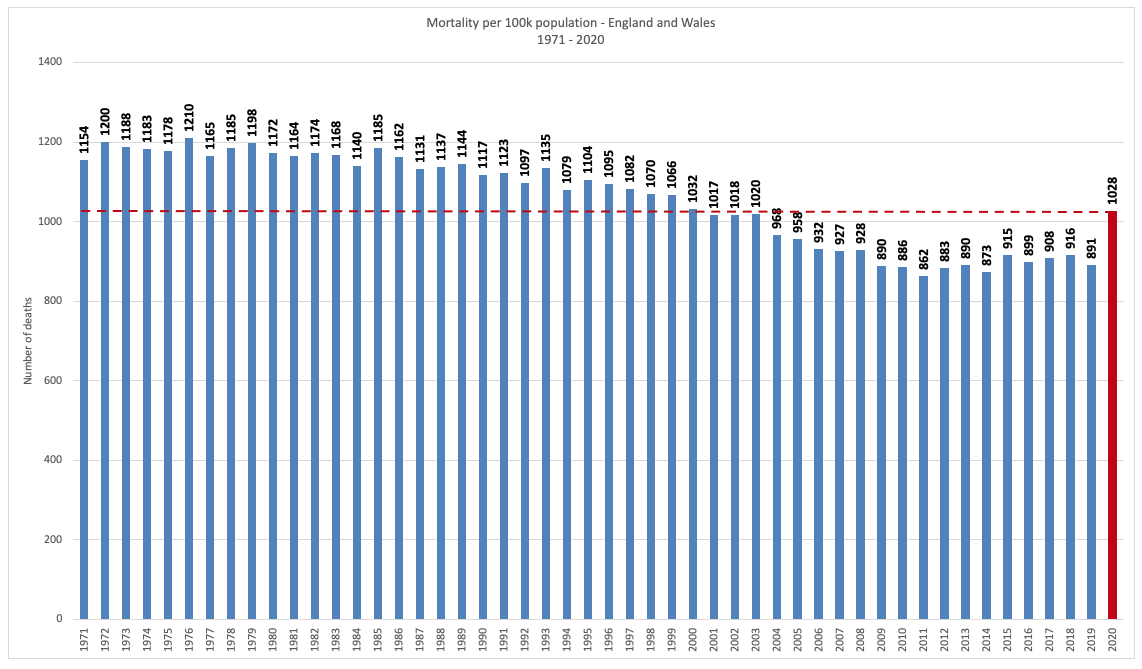 Source: Alliance for Natural Health (Data: Office of National Statistics)
Source: Alliance for Natural Health (Data: Office of National Statistics)
Again, if 2020 was an emergency then all years from 1971 to 2000 were presumably also emergencies. Next, we'll look at 2020 on a month by month basis and see what actually happened.
3. All Cause Mortality (Deaths) of English & Welsh Residents 2017 - 2020

Clearly, something happened in April 2020; the one obviously anomalous month, but equally clearly it was largely over by mid-May. How many of these deaths were avoidable and could have been treated with field-tested protocols which doctors across the world were crying out to implement (and in freer jurisdictions, were implementing, often with impressive results) and how many were the result of policy is yet to be determined and something for a tribunal or a trial (of the Nuremberg kind).
Some of these deaths in April were the result of care homes being seeded with COVID-19 patients (i.e. hospitals prematurely transferring infected patients back into care homes); the inappropriate use of ventilators (65% to 80% [NY] of COVID-19 patients die when mechanically ventilated), hospitals turning away or not responding to non-COVID-19 emergencies and people made so afraid by mainstream media coverage and government messaging that they were too scared to visit the hospital when sick. There are likely many deaths that cannot be attributed solely to SARS-CoV-2 infection that compound this April spike and these are often referred to as "lockdown deaths" (i.e. deaths related to the government's response to the virus).
The rising mortality in November and December shouldn't surprise anyone after the government imposed increasingly draconian, hope-sapping lockdowns on an already beleaguered and frustrated population, having made 70,000 households homeless, bankrupted businesses, destroyed incomes and restricted medical procedures, screenings and checkups for non-COVID-19 patients. The BMA estimates that between April and November 2020 there were 2.57 million less elective procedures and 18 million less outpatient attendances.
Now let's pull this all together, and to make sure we're comparing like-for-like we'll apply the WHO's age-standardized mortality rate (a weighted average of the age-specific mortality rates per 100,000). This is an update (see bottom of the article for details), so we can see all the way up to June 2021.
4. Age Adjusted (WHO) All Cause Mortality (Deaths) in England: 2001 - June 2021
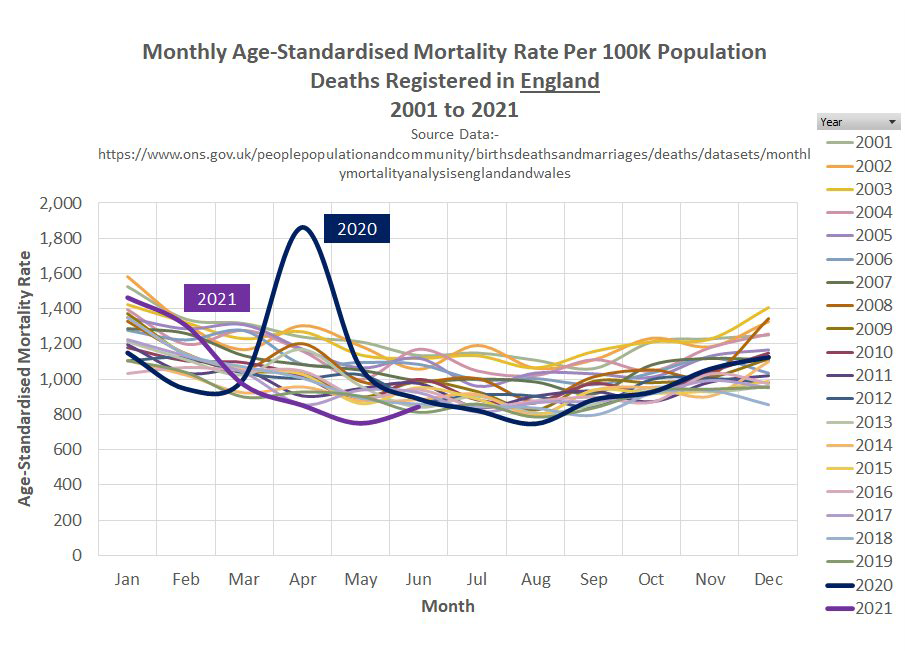 Source: Stuart Allan
Source: Stuart Allan
English deaths from COVID-19 clearly peaked in April 2020 and by June of that year any "emergency" classification had no legitimate basis; the entire "vaccine" roll-out under "emergency use authorisation" was illegitimate (and frankly not lawful).
Aside from the April 2020 bump (much of which can be explained by the response to the "outbreak"), the SARS-CoV-2 "pandemic" year, when compared to all other years looks anything but extraordinary, and nothing like the desperate picture painted by the mainstream media.
This is also born out by the NHS bed occupancy data ...
5. Hospital Bed Occupancy in England (Year-End 2019 vs 2020)
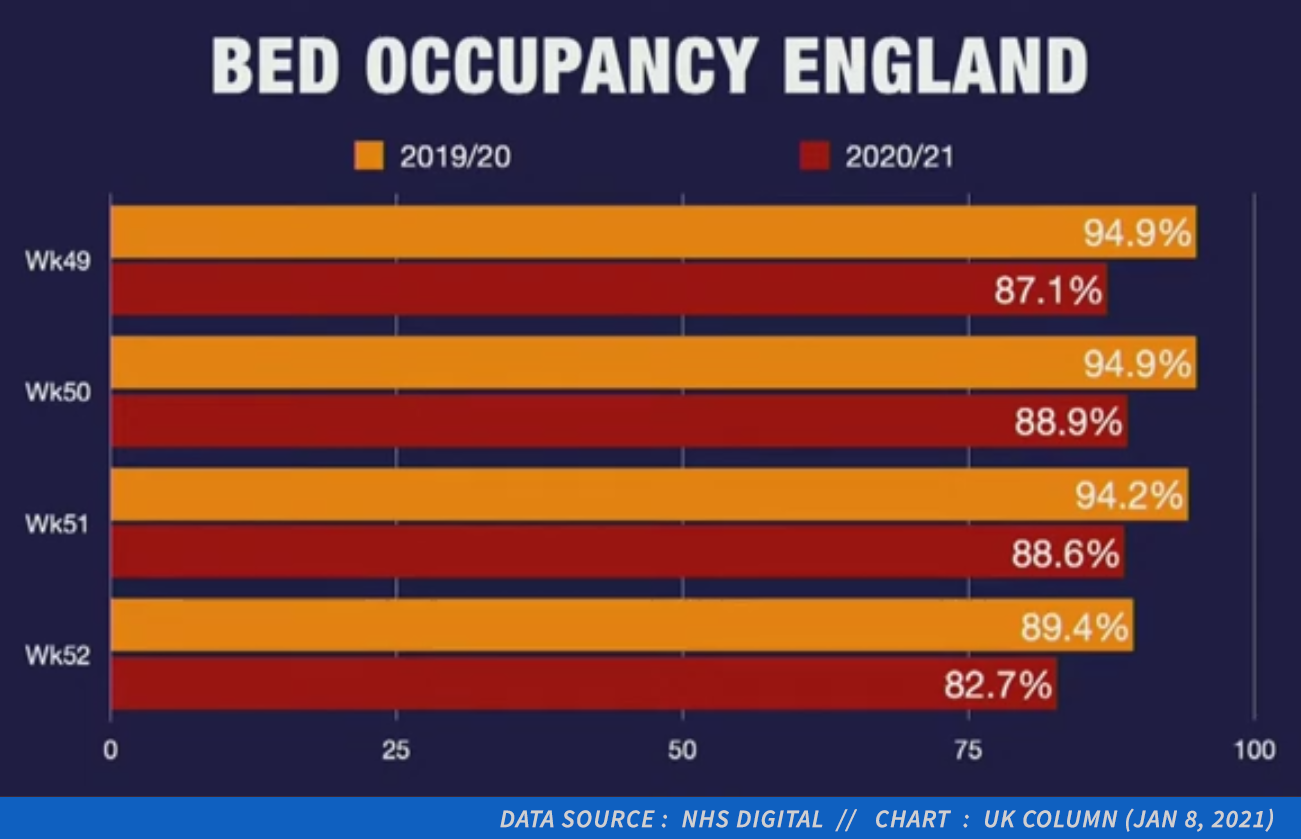 Source: UK Column News, 11/01/2021 (@ 22:20)
Source: UK Column News, 11/01/2021 (@ 22:20)
It's worth keeping in mind, that between 2010 and 2017 hospital beds were reduced by 70,000 in the UK. Any current shortage of NHS capacity is largely the result of government policy, not a coronavirus.
According to the Guardian (as this sequence @ 49:45 from UK Column News, 08/01/21 shows) the NHS has been at breaking-point every year since at least 2012. So, again I'm struggling to see an unprecedented emergency. At this point it's worth posing the question:
If the mainstream media weren't playing COVID-19 every day; if there were no lockdowns or mask mandates and if we weren't mass "testing" for SARS-CoV-2, would we really know we were in the grip of a deadly pandemic?
The final graph in this section may provide some clues as to why so many believe we are.
6. Deaths (All Causes) in England & Wales vs COVID-19 "Cases" (+PCR Tests)

Dr Malcolm Kendrick summed up the "pandemic" in his year-end review of COVID-19, "What is left to say?" (30/12/20):
It started in late March and was pretty much finished by mid-May. [...] Two things stand out. First, there was an obvious ‘COVID19 spike’. Second, what we are seeing at present does not differ greatly from previous years. The normal winter spike in deaths [...] It seems to be around the same size as winter 2017/18.
Many (at least those not pimping vaccines or pushing political agendas) agree: if there was a critical emergency, it was over in mid-May. What persists are policies serving powerful interests and positive PCR tests that enthusiastic proponents of "the pandemic" like to call "cases" (they are not cases by any standard definition, more on this in a moment).
Ultimately, all roads lead to a technology called Reverse Transcription Polymerase Chain Reaction (RT-PCR). The PCR test has become the tool of choice when you need to dial in, crank up and wind down a global "pandemic"; used nefariously, the RT-PCR is a pandemic machine. So what is RT-PCR and how does it work?
5) RT-PCR, The Pandemic Machine
1. What is PCR?
Kary Mullis won the Nobel prize for Chemistry for his invention of a process known as polymerase chain reaction (PCR), in which "a small amount of DNA can be copied in large quantities over a short period of time". The replication is done in cycles where each cycle doubles the quantity of genetic material; the number of cycles it takes to produce something identifiable is called the “cycle threshold", often referred to as the “Ct value”.
When working with RNA (corona viruses are RNA viruses), the RNA is first transcribed in reverse into its DNA complement by a reverse transcriptase enzyme; thus Reverse Transcription PCR (RT-PCR).
In their January 2020 publication “Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR” authors Victor Corman and Christian Drosten presented a diagnostic workflow and RT-qPCR protocol for the detection and diagnosis of SARS-CoV-2.
This was to become the infamous PCR test used throughout the world to "detect" SARS-CoV-2 infection.
2. What is a Case?
In 2014, commenting on the 2003 SARS [1] outbreak, Christian Drosten said:
"During the [2003] SARS [severe acute respiratory syndrome] outbreak, there was a strict case definition. People who had had contact with SARS patients but showed no symptoms were not tested with PCR. Instead they were tested for antibodies later, to see if an infection had happened. That should happen now in Saudi Arabia, too. Asymptomatic people should not be tested with PCR."
A case (unless you're promoting a pandemic) = symptoms + a positive test (often followed by a reliable confirmatory test).
In a paper titled "Diagnosing COVID-19 infection: the danger of over-reliance on positive test results (PDF)", the authors point out:
"Because of the known problems with PCR testing over many years, the WHO and the US CDC recommended for all the previous epidemics this century – SARS1, MERS, Ebola, and Zika – that:
Furthermore single test results were considered insufficient for public health decision making".
- PCR should only be used in patients with a high suspicion of having the disease or being exposed to it.
- The test must be confirmed by a different form of test, or at least by a repeat test from a different laboratory.
The current "pandemic", isn't a "casedemic" as many critics have called it; the majority of "cases" aren't cases. Instead we have an epidemic of false positive PCR results. Karry Mullis made clear, PCR was never a diagnostic tool:
"[...] with PCR, if you do it well, you can find almost anything in anybody.”
3. PCR Amplification Cycle Threshold (Ct) & False Positives
PCR works via amplification cycles. So for an RNA virus like SARS-CoV-2, the lower the cycle threshold (Ct) the greater the amount of RNA per sample and vice versa: high Ct = less RNA. Note also, that PCR does not "distinguish between infectious virus and non-infectious nucleic acid".
In "Viral cultures for COVID-19 infectious potential assessment – a systematic review", the authors point out that:
"Two studies reported the odds of live virus culture reduced by approximately 33% for every one unit increase in Ct. [...] Complete live viruses are necessary for transmission, not the fragments identified by PCR. [Tests run] with a high cycle threshold are unlikely to have infectious potential".
Swiss Policy Research in "The Trouble With PCR Tests (24/10/20)" reference the work of professor Raoult who demonstrated the risk of false positives when testing for SARS-CoV-2 in culture:
The research group of French professor Didier Raoult has recently shown that at a cycle threshold (ct) of 25, about 70% of samples remained positive in cell culture (i.e. were infectious); at a ct of 30, 20% of samples remained positive; at a ct of 35, 3% of samples remained positive; and at a ct above 35, no sample remained positive (infectious) in cell culture.
This means that if a person gets a “positive” PCR test result at a cycle threshold of 35 or higher (as applied in most US and many European labs), the chance that the person is infectious is less than 3%. The chance that the person received a “false positive” result is 97% or higher.
So at a Ct of 35 we have a 97% false postive rate. Every additional cycle further reduces the probability of there being live virus by approximately 33%. Clearly, if one wanted an accurate accounting of the number of genuine infectious cases in the real world, you'd test symptomatic people, you'd set the Ct at 30 (max) and you'd record each PCR test's Ct value. However, if you wanted to create as many symptom-free "cases" as worldly possible you'd set a maximum Ct threshold above 35 and test as many people as you could find.
[...] most commercial tests can run up to 40 to 45 CT and those who receive positive test results are not told the CT value that triggered the positive result. [...] A positive result with a high CT value will be detecting viral fragments or bits of closely related virus like the common cold that have no ability to infect another person. (source: Alliance for Natural Health)
This is why (outside the mainstream media) we see headlines like: "Portuguese Court Rules PCR Tests “Unreliable” & Quarantines “Unlawful” and "For The First Time, A US State Will Require Disclosure Of PCR 'Cycle Threshold' Data In COVID Tests" And just recently, the W.H.O (who knew all along that this was the case) just "discovered" there might be a false positive issue with PCR. They state:
Users of RT-PCR reagents should read the IFU carefully to determine if manual adjustment of the PCR positivity threshold is necessary to account for any background noise which may lead to a specimen with a high cycle threshold (Ct) value result being interpreted as a positive result.
This is the same W.H.O that recommended a Ct of 45, meaning, to quote the inventor, you will "find almost anything in anybody".

4. The Corman-Drosten RT-PCR: "Useless Test" Yields Meaningless Data
The Corman Drosten Review's Report and Addendum are worth reading for anyone who still believes the SARS-CoV-2 PCR test is fit for purpose. Its authors conclude:
In light of our re-examination of the test protocol to identify SARS-CoV-2 described in the Corman-Drosten paper we have identified concerning errors and inherent fallacies which render the SARS-CoV-2 PCR test useless.
For those who may find the Corman Drosten Review overly technical or heavy-going, Kevin McKernan provides an excellent outline of the PCR technology and its issues when used as a diagnostic tool in an interview called "PCR testing insights" (which you can watch online at PCRClaims, or download in MP4 format). Additionally, Dr Sam Bailey provides a concise and equally thorough examination in her video "The Truth About PCR Tests".
The SARS-CoV-2 PCR test is indeed "useless", or more politely "not fit for purpose" and more importantly, it's producing results that are meaningless. This is vital, since all (so-called) "public health policy", from social distancing, to mask mandates, to lockdowns, to travel bans, to quarantines and now, experimental and unlicensed "vaccines", are based on the Corman-Drosten RT-qPCR test. A PCR test that was never peer-reviewed and as Mary Holland, General Counsel of Children's Health Defense pointed out (@ 12:50) is also an unlicensed and emergency use product:
"[...] these novel mRNA vaccines which most scientists we're listening to say are not really vaccines [...] This is experimental and that's what the EUA (Emergency Use Authorization) designation means. [...] Right now we have very strong grounds to push back against any efforts to force people to take these vaccines or even the test. The PCR test for COVID is also an EUA product; it has not been licensed for its purpose [...] it is experimental by definition."
5. The Data are False, The Consequences are Real
The damage that has been caused by this incarnation of the PCR test is almost incalculable. But perhaps most worrying is what this means for the "vaccine" experiment that is currently underway.
The vaccine trials rely on the same SARS-CoV-2 PCR test that has: a) been shown to be so flawed as to be utterly "useless"; b) uses a technology that was never intended as a diagnostic tool; and c) was run at Ct values that would provide meaningless results.
All trial data is based on how trial participants tested:
- How many in the "vaccine" group tested positive for SARS-CoV-2 versus how many in the placebo group?
- How did the symptoms of the vaccinated group compare with the symptoms of the non-vaccinated group when participants tested positive (via PCR) for SARS-CoV-2?
If we cannot trust the test upon which all claims of the COVID-19 "vaccines" are based, then we literally know nothing about the efficacy of these experimental "vaccines". We are beginning to find out about their safety however, and frankly I worry for the long term health of every single participant in this ongoing trial.
Ultimately, the real experiment is between the compliant and ill-informed (the vaccinated group) and the non-compliant and well-informed (the control). I'm not looking forward to the results when the trials end in 2023.

6) The Asymptomatic Spreader
There's almost nothing right about the caption on the Tier 3 Alert below (click to enlarge), which reads:
"Around 1 in 3 people with Covid-19 have no symptoms, so will be spreading the virus without realising."

An informed person would look at this and likely muse: "a 33% false-positive rate seems a little low". The sign should of course read:
"Around 1 in 3 people with Covid-19 have no symptoms because they don't have Covid-19."
COVID-19 is the disease. The conflation of the disease with the virus has led many to believe that the "vaccine" prevents infection and transmission of the virus; when in reality the manufacturers claim their "vaccines" merely dampen symptoms of the COVID-19 disease; effectively turning the "vaccinated" into asymptomatic spreaders (which ironically is what the sign is warning you about).
If you were asymptomatic while actually infected with SARS-CoV-2, that would imply your immune system dealt with the infection and prevented the disease state called COVID-19. Peter Doshi in a BMJ article (17/09/20) titled "Covid-19: Do many people have pre-existing immunity?" makes the case that T-Cell cross-immunity from other coronaviruses was likely prevalent in most populations before SARS-CoV-2 arrived:
In a study of donor blood specimens obtained in the US between 2015 and 2018, 50% displayed various forms of T cell reactivity to SARS-CoV-2
So, let's talk about the near mythical "asymptomatic spreader".
Dr Clair Craig in a BMJ Rapid Response to "Mass testing for covid-19 in the UK" wrote:
"Mass testing and accompanying harmful lockdown policies are justified on the assumption that asymptomatic transmission is a genuine risk. [...] However, the only word which can be used to describe the quality of evidence for this is woeful."
In a video titled: "Dr Clare Craig - The trouble with PCR" (which you can watch online at PCRClaims, or download in MP4 format), Dr Craig covers a number of problems with the PCR test that have not been addressed here, she also looks at the Lateral Flow Tests, the death certification issue, and finishes by destroying the mythology around the asymptomatic spreader. I can't put it any more concisely or eloquently than her, so I'll simply recommend you watch the full interview.
What is surprising, is just how scant the evidence for the asymptomatic spreader actually is. In their BMJ pre-print titled "Has the Evidence of Asymptomatic Spread of COVID-19 been Significantly Overstated", Dr Craig and Jonathan Engler (MBChB LLB) state:
The existence of transmission of SARS-CoV-2 from asymptomatic individuals has become an accepted truth but the evidence for this phenomenon being anything other than mistaken interpretation of false positive test results is weak. Examination of the underlying data from the most frequently-cited such meta-analyses reveals that the conclusions are based on a surprisingly small number of cases (six in total globally) and, moreover, the possibility that they are all coincidental contacts with false positive results cannot be ruled out.
The only thing I will add is this. The idea of the asymptomatic spreader appears to have been egregiously over-stated. It's an important idea and worthy of promotion, if your goal is to make everyone afraid of everyone else.
7) A Viral PR Machine
A Brief History
It's not like we haven't been here before. The prelude to the SARS-CoV-2 "pandemic" was the H1N1 Swine Flu "pandemic" of 2009, in which some familiar names (Fauci, Ferguson, Imperial, W.H.O) used PCR testing to create a second wave ("around a year after the virus had more or less disappeared") which was light on hospitalisations and deaths but heavy on "cases".
 Failing upwards: The Bill & Melinda Gates Foundation reward key pharmaceutical industry propagandists for their impressive "mistakes".
Failing upwards: The Bill & Melinda Gates Foundation reward key pharmaceutical industry propagandists for their impressive "mistakes".
The W.H.O altered their definition of a “pandemic” to create sufficient panic to sell billions of doses of untested flu vaccines. CHD explains what happened next:
The [W.H.O's] declaration of H1N1 as a pandemic launched $18 billion worth of “dormant” flu vaccine contracts, and allowed GSK to push its vaccine, Pandemrix, onto countries all over the world. The Pandemrix vaccine caused severe, life-long, adverse neurological reactions, including narcolepsy and cataplexy (the sudden, brief loss of voluntary muscle tone triggered by strong emotions), in at least 1,300 children across Europe. It’s possible even more children were injured, as it’s estimated that only 10% of adverse reactions are reported through national adverse event reporting systems.
Fast Forward to 2020
- Feb 17th 2020 - Fauci stated: "risk of coronavirus in USA is miniscule"
- Feb 28th 2020 - Bill Gates warned coronavirus may be the "once in a century pathogen we've been worried about"
- March 4th 2020 - CDC issues new guidlines for certifying COVID-19 deaths [PDF]
The CDC's new certification guidelines stated:
"It is important to emphasize that Coronavirus Disease 2019 or COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death. [...] Specification of the causal pathway leading to death in Part I of the certificate is also important. For example, in cases when COVID-19 causes pneumonia and fatal respiratory distress, both pneumonia and respiratory distress should be included along with COVID-19 in Part I."
This is important, as Part 1 of the death certificate enters into the data / statistical record. Institutions across the globe were strongly incentivised to mark the bottom line (the underlying cause) as COVID-19. Thus the root cause of death was heavily skewed toward COVID-19, amplifying the impact of the SARS-CoV-2 virus and its pathology.
Italy’s COVID-19 Surveillance Group (part of the National Institute of Health) issued a report in late March 2020 about which Professor Walter Ricciardi (scientific adviser to Italy’s minister of health) commented:
"The way in which we code deaths in our country is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus […] On re-evaluation by the National Institute of Health, only 12 per cent of death certificates have shown a direct causality from coronavirus, while 88 per cent of patients who have died have at least one pre-morbidity – many had two or three”.
This resulted in some bizarre data anomalies in the medical reporting systems. For example, sentinel hospitals (part of a network of institutions that report health surveillance and admissions data back to the CDC), reported that hospitalisations due to influenza had flat-lined in 2020.

Either COVID-19 cures influenza or we have a serious administration problem. Let's turn to the W.H.O to see if this peculiar phenomenon is mirrored globally.
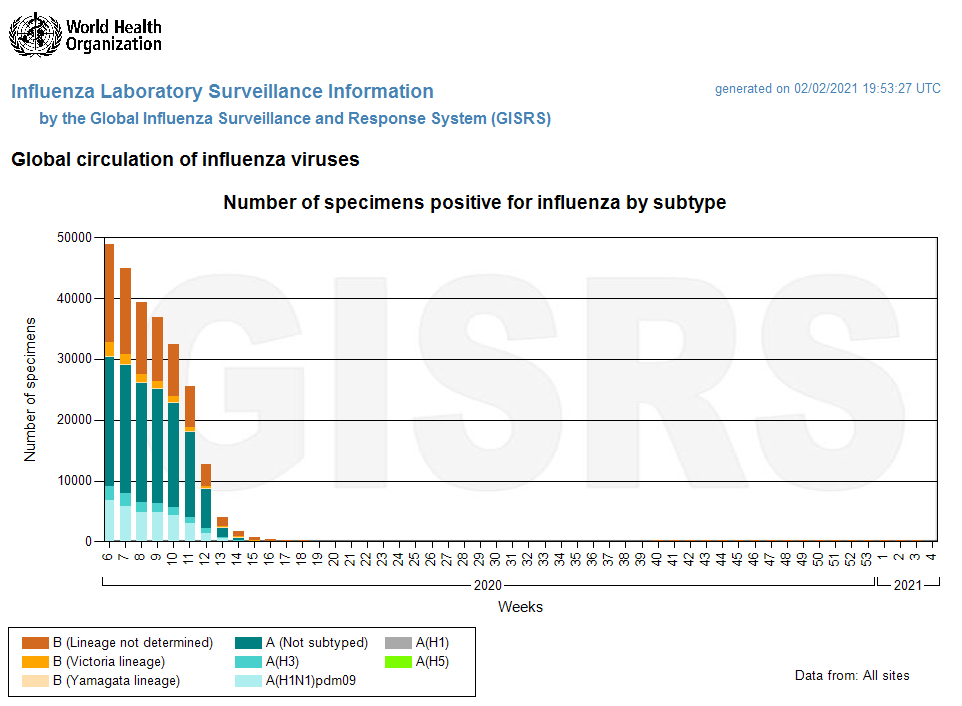 Source: snapshot of W.H.O's FluNet live data (02.02.21)
Source: snapshot of W.H.O's FluNet live data (02.02.21)
Such "anomalies" have not gone unnoticed and many are (and have been) calling for an audit of the death certifications during the COVID "pandemic". The mis-attribution of deaths to COVID-19 (presumably to amplify the perceived threat) has resulted in a corresponding drop in deaths from flu, pneumonia, emphysema and chronic pulmonary disease. This and mass PCR testing are covered in a short film by Jeffrey Peel called "A Tale of 2 Januarys" which looks at the very similar UK mortality rates of January 2015 (a non-"pandemic" year) and January 2021.
Viral Public Relations
From the very beginning the mainstream media were "all-in", providing an incessant, breathless "coverage" of the "pandemic", from the dashboards that popped up almost instantaneously, to the early "harrowing" YouTube videos of Hubei residents falling flat on their faces as they dropped dead in the street in front of lucky amateur videographers (a phenomenon that didn't travel well it seems). All this was captured early on by Off-Guardian in a February 2020 piece titled "Media Whipping Covid19 Panic to Unprecedented Heights". If the media were hyperbolic then, they soon went into warp drive and never looked back.
Qui Bono
China, the totalitarian state-capitalist poster-child of the World Economic Forum, was the only major economy to report positive GDP growth in 2020. They initiated the repressive "lockdown" policies that so impressed, and were mimicked by, authoritarians around the globe to devastating effect. The true costs (in terms of the economy, health, education, etc) of these policies were outlined by Dr. Scott Atlas in an interview on the theme: "The Efficacy of Lockdowns, Social Distancing and Closings" (well worth a watch if you believe the "cure" has not been far, far worse than the disease).
In terms of nations, China likely stands alone, but when it comes to more specific beneficiaries, I'll refer you to an interesting peer-reviewed paper on this very subject, published in the International Journal of Vaccine Theory, Practice, and Research, titled "Planned Surveillance and Control by Global Technocrats: A Big-Picture Look at the Current Pandemic Beneficiaries" [Full PDF].
8) The Future Died In Someone's Past (Collateral "Vaccine" Damage?)
On December 1st 2020, Dr. Michael Yeadon (former CSO at Pfizer) and Dr. Wolfgang Wodarg filed a legal petition [PDF download] with the European Medicines Agency requesting an emergency "stay of action" for all ongoing clinical trials of COVID-19 vaccines. A similar petition was filed by Dr. Sin Hang Lee and the Informed Consent Action Network (ICAN) in the U.S. [PDF download].
The "Knowns" and the "Known Unknowns"
In the Yeadon-Wodarg filing (under Section C. Statement of Grounds), there are some insights as to the potential immediate, short and medium term dangers that may lie ahead (on top of the reported deaths and traditional side effects mentioned on the FDA's "safety surveillance" guidelines, see Part 3).
Early on they cite the same flawed PCR problems (pointed out above in Part 5) stating:
[Section C. III] If the assignment of cases and non-cases during the course of the trials is not accurate, the vaccines will not have been properly tested. If the vaccines are not properly tested, important public policy decisions regarding its use will be based on misleading evidence.
In sub-section VIII, they discuss the issue of Antibody Dependent Enhancement (ADE), sometimes inaccurately referred to as Immune Dependent Enhancement (IDE). Authors Cardozo and Veazey stated (in their paper, "Informed consent disclosure to vaccine trial subjects of risk of COVID‐19 vaccines worsening clinical disease", 28/10/20): "the risk of ADE in COVID‐19 vaccines is non‐theoretical and compelling".
In an attempt to create a vaccine for 2003's SARS1, the pharmaceutical industry succeeded in stimulating a robust anti-body response in their animal trials, however when challenged with the wild virus, many of the trial animals suffered an acute reaction caused by ADE and died. ADE via vaccination may cause idiopathic antibodies that act like a Trojan horse for the wild virus, allowing the target virus to enter cells and replicate:
[Section C. VIII] In some viruses, if a person harbors a non-neutralizing antibody to the virus, a subsequent infection by the virus can cause that person to elicit a more severe reaction to the virus due to the presence of the non-neutralizing antibody. This is not true for all viruses, only particular ones. This is called Antibody Dependent Enhancement (ADE), and is a common problem with Dengue Virus, Ebola Virus, HIV, RSV, and the family of coronaviruses. In fact, this problem of ADE is a major reason why many previous vaccine trials for other coronaviruses failed. Major safety concerns were observed in animal models. If ADE occurs in an individual, their response to the virus can be worse than their response if they had never developed an antibody in the first place. This can cause a hyperinflammatory response, a cytokine storm, and a generally dysregulation of the immune system that allows the virus to cause more damage to our lungs and other organs of our body. In addition, new cell types throughout our body are now susceptible to viral infection due to the additional viral entry pathway. There are many studies that demonstrate that ADE is a persistent problem with coronaviruses in general, and in particular, with SARS-related viruses.
Sub-section IX would appear to question the status of these "vaccines" as vaccines:
[Section C. IX] There are some concerning issues with the trial designs, spelled out by Dr. Peter Doshi in the British Medical Journal. Dr. Doshi focuses on the two biggest issues. First, none of the leading vaccine candidate trials is designed to test if the vaccine can reduce severe COVID-19 symptoms, defined as: hospital admissions, ICU or death. And, second, the trials are not designed to test if the vaccine can interrupt transmission (https://www.bmj.com/content/bmj/371/bmj.m4037.full.pdf). If neither of these conditions is met, the vaccine in essence performs like a therapeutic drug [...]
Sub-section X deals with the anaphylactic shock issue that Children's Health Defense warned the FDA about on 5th September 2020.
[Section C. X] In the Pfizer/BioNTech mRNA vaccine candidate, polyethylene glycol (PEG) is found in the fatty lipid nanoparticle coating around the mRNA. Seventy percent of people make antibodies to PEG and most do not know it, creating a concerning situation where many could have allergic, potentially deadly, reactions to a PEG-containing vaccine.
Sub-section XI is perhaps the most troubling. It deals with the lack of testing around fertility, the latency in fertility issues arising, and a potential method of action for COVID-19 "vaccines" to result in sterility:
[Section C. XI] Several vaccine candidates are expected to induce the formation of humoral antibodies against spike proteins of SARS-CoV-2. Syncytin-1 (see Gallaher, B., “Response to nCoV2019 Against Backdrop of Endogenous Retroviruses”), which is derived from human endogenous retroviruses (HERV) and is responsible for the development of a placenta in mammals and humans and is therefore an essential prerequisite for a successful pregnancy, is also found in homologous form in the spike proteins of SARS viruses. There is no indication whether antibodies against spike proteins of SARS viruses would also act like anti-Syncytin-1 antibodies. However, if this were to be the case this would then also prevent the formation of a placenta which would result in vaccinated women essentially becoming infertile.
To my knowledge, Pfizer/BioNTech has yet to release any samples of written materials provided to patients, so it is unclear what, if any, information regarding (potential) fertility-specific risks caused by antibodies is included. According to section 10.4.2 of the Pfizer/BioNTech trial protocol, a woman of childbearing potential (WOCBP) is eligible to participate if she is not pregnant or breastfeeding, and is using an acceptable contraceptive method as described in the trial protocol during the intervention period (for a minimum of 28 days after the last dose of study intervention). This means that it could take a relatively long time before a noticeable number of cases of post-vaccination infertility could be observed.
The UK government, in their "Reg 174 Information For UK Healthcare Professionals [PDF]", states that "reproductive and developmental toxicity were investigated in rats" but the potential impact on fertility in humans has not been tested and is thus unknown.
The COVID-19 "vaccines" work by encoding for a spike protein. In biology, form is function, and proteins gain their form via a process called "folding"; the sequence of amino acids in a protein is sufficient to determine its three-dimensional structure and via Brownian motion proteins "fold" into their pre-specified form. However, proteins can, and do, mis-fold and mis-folded proteins in neurons are implicated in disorders such as Parkinson's and Altzheimer's. This short interview with neuroscientist Dr. Chris Shaw looks at previous mRNA vaccine studies which showed that the lipid "vector" or "construct" (the delivery mechanism for the mRNA) and the mRNA itself were not being contained in the target cells and instead made their way to a range of organs including the brain.
So much is unknown regarding the long term effects of these "vaccines", that we won't truly comprehend the true cost of this vast human experiment until long after the trials complete in early 2023.
Light at the End of the Tunnel (Crimes & Revelations)
Let's circle back to where we almost began, with Iain Davis in his article "What Vaccine Trials?":
"The degree to which people have been misled into believing that these vaccines are known to be either safe or effective is almost beyond imagination."
The same could be said for how the public have been misled over the course of this entire "pandemic". The primary tool in this criminal deception has been the Corman-Drosten RT-qPCR test - the pandemic machine.
We'll end with two questions:
- Why have these experimental vaccines been pushed so aggressively?
- What if the COVID-19 story doesn't end with a vaccine, but actually contains within it the end of vaccines;
a new paradigm in the treatment of viral diseases generally [PDF]? . . .
Source: The Highwire, 29/01/21
Last Updated: 31/07/21
Changelog: Amendments, Corrections, Additions
- Amendment (31/07/21): Replaced the InProportion2 cumulative comparison of 2000 and 2020, with an up-to-date Age Standardised (WHO) monthly comparison for 2001 to June 2021.
- Amendment (14/05/21): Reinstated the link to Rancourt's mask RCT analysis after Baruch Vainshelboim's comprehensive Stanford review was "retracted" / censored at the publisher's (Elsevier) request.
- Amendment (25/04/21): Replaced a link to Dr Merrit's paper "The Treatment of Viral Diseases: Has the Truth Been Suppressed for Decades?" (which is also available in Part 8) with a link to c19early.com (a real-time database and meta analysis of hundreds of studies for COVID-19 therapeutics)
- Amendment (25/04/21): Replaced a link to Rancourt's mask RCT analysis with Baruch Vainshelboim's comprehensive Stanford review called "Facemasks in the COVID-19 era"
- Addition (16/02/21): Added a link to Dr Sam Bailey's "The Truth About PCR Tests"
- Addition (12/02/21): Added a link to the paper "Informed consent disclosure to vaccine trial subjects of risk of COVID‐19 vaccines worsening clinical disease" on the topic of ADE
- Addition (09/02/21): Added a link to the known ingredients of each of the main COVID-19 "vaccines"
- Addition (04/02/21): Added a brief paragraph on T-Cell cross immunity in relation to asymptomatic infections
- Addition (03/02/21): Added link to the film by Jeffrey Peel called "A Tale of 2 Januarys"
- Addition (03/02/21): Added W.H.O's global circulation of influenza viruses graph for 2020
- Correction (02/02/21): 70,000 ICU beds has been changed to 70,000 hospital beds
- Addition (02/02/21): Added link and quote from the pre-print: "Has the Evidence of Asymptomatic Spread of COVID-19 been Significantly Overstated?"